Paving the Way for a Career in High Value Care: A Roadmap for Future Clinician Leaders

Abstract
The healthcare cost crisis in the USA has become unsustainable, with patients facing rising premiums and deductibles and providers unable to meet their bottom lines, forcing practice mergers and buyouts that further exacerbate gaps in care access. Promoting high value care has been a stated priority of health systems for nearly two decades, but practical implementation within a largely fee-for-service system has remained limited. Practicing clinicians must be at the forefront of health system transformation in order to promote value, but medical trainees and early career physicians—who have an increasing interest and knowledge in high value care—often lack a structured career path to lead change in this space. Trainees and early career faculty would benefit from practical and concrete guidance throughout their training to ensure they can sustain their passion and leadership in this space as they transition to faculty/independent practice. We outline four career pathways—Education, Care Delivery Research, Quality/Operations Leadership, and Commercial Innovation—that can help trainees translate early interest in high-value care into sustainable professional roles. Creating visible, supported pathways for these careers is essential if health systems hope to retain and empower the next generation of clinicians committed to advancing value.
BACKGROUND
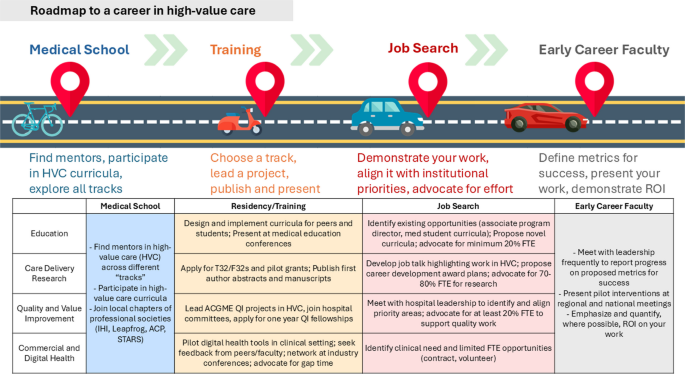
With rising healthcare costs increasingly placing strain on clinicians, health systems, and patients’ out-of-pocket spending, there is an urgent need to develop, test, and scale high-value care (HVC) models. Over the past decade, there has been an increasing emphasis on teaching HVC principles in medical training, creating a new generation of cost-conscious clinicians ready to transition to practice with fresh perspectives, energy, and ideas about transforming care delivery.1,2 Medical training is a formative time to generate ideas given clinicians serve as frontline providers and witness gaps in quality or high cost practices regularly. However, despite the increasing interest and knowledge of HVC among early career clinicians, the road to integrating these principles into a clinical career is poorly defined and often not clearly visible for aspiring leaders and change agents. Structural barriers including lack of clearly specified promotion pathways, limited funding streams, and a dearth of established job titles make navigating these career paths opaque for young health professionals. Furthermore, structured programs to promote value-oriented practices—such as Choosing Wisely—have diminished in capacity or faded recently,3 further eroding the landscape for opportunities for national recognition and career growth for this essential work. Yet there are examples of faculty who have forged successful career paths focused on HVC in education, care delivery research, health system leadership, and commercial innovation. In this perspective piece, we provide a concrete roadmap (Fig. 1) and illustrative examples to help trainees and early faculty members to chart a path that can transform their dedication to promoting HVC into an impactful and sustainable career. These pathways are not mutually exclusive, and many successful careers blend elements across domains.
MEDICAL EDUCATION
Dr. Cutcosts is an associate professor and general surgeon and leads a HVC curriculum for surgery residents. After establishing a track record of successful medical education initiatives, including a growing publication record, she secured 20% protected effort over time for her teaching responsibilities. She helps residents develop and publish projects ranging from antibiotic stewardship to use of non-disposable equipment to de-implementation of unnecessary pre-operative testing.
Efforts to incorporate HVC into medical training have grown substantially over the last decade. The Accreditation Council for Graduate Medical Education (ACGME) requires cost awareness and health systems science to be part of the systems-based practice core competency for all accredited residency and fellowship programs.4 This requirement provides a key opportunity for institutions to hire and invest in faculty who can teach these principles, ranging from de-escalation of diagnostic tests to improved cost conversations with patients. Trainees can partake in programs like STARS (Students and Trainees Advocating for Resource Stewardship)—specifically geared towards medical students—and organizations such as the Institute for Healthcare Improvement (IHI) and American College of Physicians (ACP), as well as local institutional HVC interest groups. These latter organizations often provide opportunities across the career continuum, starting from undergraduate/pre-medical phase to early career faculty to advance HVC in medical education.1,2 Trainees and early career faculty can direct ongoing training through educational programs such as the Value-Based Care Academy at Stanford University School of Medicine5 and the American Medical Association (AMA) Value-Based Care Modules,6 among others, which provide continuing medical education (CME) credit geared towards faculty and colleagues. Successful early career medical professionals interested in becoming HVC clinician educators for trainees or peers seek mentorship in medical education and become involved in curricula development early in medical school, leveraging existing resources. For example, Costs of Care and ACP have online modules7,8 for HVC and leading cost conversations that are specifically geared towards trainee education and may serve as a useful blueprint upon which to build a medical student curricula. Trainees interested in promoting HVC through medical education may also consider applying for QI-specific chief resident roles such as the national VA Chief Quality and Safety (CRQS) and/or medical education fellowships which often include funded master’s level training in education. Trainees can additionally build their networks and share ideas around HVC education initiatives through presenting at national conferences geared towards medical educators and value, such as the annual IHI forum and annual Society of General Internal Medicine (SGIM) meeting, and publishing in premier medical education journals.
CARE DELIVERY RESEARCH
Dr. Quality is a medical oncologist at a Veterans Affairs (VA) hospital and conducts research on the impact of telehealth on cancer outcomes. They secured a VA career development award early in their career and continue to apply for larger grants to support their work. They see patients in clinic one morning per week.
Many trainees aspire to develop the tools and knowledge to pilot and rigorously evaluate models of care delivery as well as demonstrate their impact on value. Such care delivery research is essential to successfully scale and disseminate successful HVC practices. Developing an identity as a HVC researcher often requires trainees to bridge traditional disciplinary silos, combining clinical insight with implementation science, policy awareness, and operational collaboration in ways not always clearly emphasized in conventional academic pathways. Successful trainees aspiring towards an academic research career in HVC seek out general academic fellowships and/or structured grants such as T32s and F32s that allow dedicated time for coursework and research training and have been shown to predict success in receipt of larger grants.9 Mentorship can be a barrier for trainees, however, in the post-covid era, virtual mentorship models have been broadened and redefined.10 Trainees now can more readily seek mentors outside of their own institution, leveraging existing communities such as the Healthcare Systems Research Network, Academy Health, and networking through subspecialty-focused health services research groups/conferences (e.g., American Heart Association Quality of Care and Outcomes Research Scientific Sessions). Trainees have also applied for pilot funding from diverse sources including government, private foundations, and where appropriate, industry partners (who increasingly generate quality or value-focused requests for proposals). Multiple free, national population-level datasets to study quality and cost can serve as useful tools to measure state-, region-, or hospital-level quality (e.g., National Committee for Quality Assurance’s Health Effective and Data Information (HEDIS) and Patient-facing Consumer Assessment of Healthcare Providers and Systems (CAHPS) datasets).11 These publicly available datasets may foster collaborations that are not reliant on institutional-level resources or mentorship. Individual payers—although seemingly an unlikely ally—maintain their own datasets and have increasing interest in studying quality, cost, and value for their members and contracted physician/hospital groups. Early career investigators focused on studying and scaling value initiatives at the delivery level would further benefit from rigorous training in implementation science, including virtual programs such as the Training Institute for Dissemination and Implementation Research (TIDIRH).12
QUALITY/OPERATIONS LEADERSHIP
Dr. Ceesuite is a pediatric hospitalist and associate chief medical officer at a large academic children’s hospital. He helps set goals for the hospital’s accountable care organization and is an associate program director for the pediatric hospitalist fellowship program. He works six inpatient weeks per year on service.
Increasingly, organizations are hiring Chief Quality or Chief Value Officers to help set high-level, strategic goals in areas that align HVC priorities across departments.13 Example activities related to value may include implementing rollout of an accountable care organization and building a high-quality affiliate network. These positions are often targeted toward mid-career clinicians, but represent a clear trajectory for early career clinicians interested in operationalizing HVC models. Students and residents interested in such roles can partake in resident/fellow quality improvement (QI) initiatives, join operational committees within the hospital, participate in one year QI fellowships (such as the VA Quality Scholars Program),14 and learn rigorous QI methodology applied to value (e.g., American Society of Clinical Oncology Quality Training Program,15 an intensive 6-month initiative with frequent participation by trainees, and Intermountain’s virtual Advance Training Program (ATP) in Clinical Quality Improvement).16 These programs help trainees sharpen their knowledge of reimbursement models specific to different practice settings and payers. Trainees can consider rotations, where available, at affiliated community sites, safety net hospitals, and VA hospitals to gain perspective on diverse approaches to the delivery of HVC. Some trainees may choose to pursue additional coursework in health systems and leadership to further develop their network and skillsets in health systems and quality.
COMMERCIAL AND DIGITAL HEALTH
Dr. Value worked in digital health prior to medical school. After her emergency medicine residency, she started a company to improve electronic health record integration, motivated by her experiences watching patients fall through the cracks due to lack of care coordination. She works on a contract basis with a local private emergency department for two shifts per month.
Clinicians are needed in the commercial and digital health sector to drive innovation in care delivery, particularly in the era of artificial intelligence, rising administrative burdens, and growing virtual care models. Technology firms and consumer health platforms (e.g., Google Health, Samsung Health, Apple)—increasingly recruit clinicians for roles in product development and clinical strategy. These platforms have the potential to develop cost-saving products (e.g., remote monitoring, AI tools for healthcare organizations). However, clinician leadership is essential to ensure these platforms are both provider and patient centric. Medical students and residents interested in this path can explore internships in the commercial space to establish relationships with engineers, product developers, and venture capitalists, join organizations and conferences with like-minded physicians (e.g., annual American Medical Association Physician Entrepreneur Forum), consider business coursework (or a full Master’s in Business Administration (MBA)) to help generate and grow ideas, and apply for pilot grant opportunities such as Small Business Innovation Grants (SBIR).17 Residents and fellows can discuss with their program directors whether traditional research or quality improvement blocks can be leveraged for networking and product building. Some platforms are partnering with healthcare delivery systems to pilot, study, and implement value-based care programs that can effectively track population level quality and cost metrics, deploy proven cost-saving care coordination initiatives such as navigators, and enable automation in administrative burdens that may ultimately be cost saving for practices. Clinicians with frontline and recent experience navigating the challenges of a rapidly changing healthcare system are essential to assess and evaluate these growing platforms with rigor, ensure integration with current clinical workflows, and ultimately implement and assess their effectiveness. Early career clinicians highly motivated to enter the digital health space may find specialties that allow for shift work more accommodating to their schedules, e.g., hospital medicine or emergency medicine, or may consider a volunteer position to maintain their clinical knowledge.
CONCLUSION
Transformation of the healthcare system has never been more urgent and increasingly medical trainees have the interest and knowledge to incorporate HVC into their careers. Trainees should proactively tailor their training and education to align with their interests and goals in HVC. In parallel, institutions and senior mentors/current leaders in HVC must elevate these passionate and activated clinicians and provide the structure, protected time, and support early in their careers to help them achieve their full potential. Professional societies can aid institutions in this support by bringing together early career clinicians to share ideas and resources, develop a community committed to thoughtful implementation of HVC, and where possible, provide funding for early career clinicians to conduct pilot work across all four pathways. Without intentional and structured career pathways, the growing pipeline of HVC-trained clinicians could disperse into traditional roles that fail to leverage their passion and expertise. As a result, practical implementation of HVC principles may remain muted. A nominal investment in early career clinicians interested in HVC has the potential to yield significant returns in curbing costs and improving outcomes for patients.
REFERENCES
1.Silverstein WK. et al. How Medical Students Benefit from Participating in a Longitudinal Resource Stewardship Medical Education Program (STARS): An International Descriptive Evaluation. J Gen Intern Med. 2025;40:146–152.
2.Born KB, Moriates C, Valencia V, Kerssens M, Wong BM. Learners as Leaders: A Global Groundswell of Students Leading Choosing Wisely Initiatives in Medical Education. Acad Med J Assoc Am Med Coll. 2019;94:1699–1703.
3.Kerr EA, Kullgren JT, Saini SD. Choosing Wisely: How To Fulfill The Promise In The Next 5 Years. Health Aff (Millwood). 2017;36:2012–2018.
4.Hackbarth G, Boccuti C. Transforming graduate medical education to improve health care value. N Engl J Med. 2011;364:693–695.
Stanford Value-based Care Academy – Stanford Med Education. https://mededucation.stanford.edu/courses/stanford-value-based-care-academy/.
Value-Based Patient-Centered Care. https://edhub.ama-assn.org/course/260.
Healthcare Transparency | Cost of Care Conversations Resources. 2022. https://www.acponline.org/clinical-information/high-value-care/resources-for-clinicians/cost-of-care-conversations.
Cost Conversations – Costs of Care. https://stars.costsofcare.org/costconversations/.
9.Ghabra S, Demblowski LA, Larrain C, Choo-Wosoba H, Zeiger MA. R01 Funding for Surgeons; What Are the Key Factors for Success? J Surg Res. 2025;312: 7–14.
10.Forster CS. et al. Perspectives from the Society for Pediatric Research: advice on sustaining science and mentoring during COVID-19. Pediatr Res. 2021;90:38–743.
Narayan A, Kocher B, Shah NR. Improving The Quality Of Quality Metrics. Health Aff. Forefr. https://doi.org/10.1377/forefront.20240315.619754.
Training Institute for Dissemination and Implementation Research in Health (TIDIRH) | Office of Behavioral and Social Sciences Research. https://obssr.od.nih.gov/training/training-supported-by-the-obssr/training-tidirh.
13.Zuchowski ML, Henzler D, Alscher MD, Nagel E. The impact of C-level positions on hospital performance: A scoping review of top management team outcomes. Health Policy. 2025;157:105346.
14.Godwin KM. et al. Value of Interprofessional Education: The VA Quality Scholars Program. J Healthc Qual. JHQ 2021;43:304.
Quality Training Program – ASCO. https://www.asco.org/meetings-education/training-programs/quality-training-program.
ATP. https://intermountainhealthcare.org/for-professionals/hdi/atp.
| SBIR. https://www.sbir.gov/.