Value-based insurance designs (VBID) set patient copayment rates based on the value of the specific clinical service to a specific patient (considering benefits and costs), rather than exclusively based on costs.1 In other words, high-value services would be provided with low (or no) out-of-pocket costs, whereas services considered low-value would be charged at a higher out-of-pocket rate.
Source: University of Michigan. Center for Value-Based Insurance Design website. Resources: infographics. Visit to learn more about V-BID, implementation, and trials of its adoption.
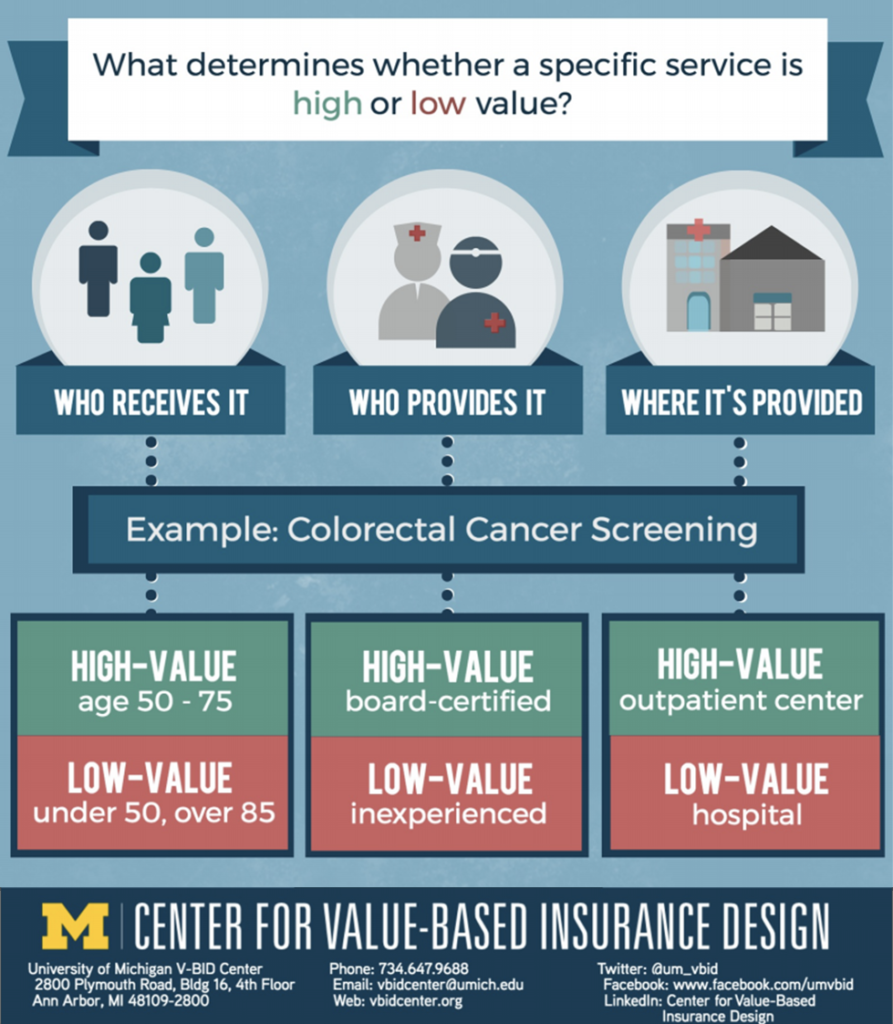
Increased cost-sharing — the amount that a patient pays towards his or her clinical services — has been shown to decrease utilization of both low- and high-value services. To combat this, V-BID suggests increased cost-sharing for low-value services (those shown to have little or no benefit) and conversely decreased cost-sharing for high-value services, with the goal of removing financial barriers. Ideally, this would be specifically targeted for each patient and their given conditions; VBID plans should be designed with clinical nuance in mind, “recognizing that the clinical benefit of a specific service depends on who receives it, who provides it, and where and when in the course of disease the service is provided.”2 This has also been called Precision Benefit Design. As precision medicine — or the tailoring of clinical services to each individual patient — advances, so does the tailoring of VBID to each patient’s needs.
For example, a patient with diabetes should undergo annual eye examinations, whereas not everybody should receive such examinations. Therefore, in properly designed VBID programs the cost sharing for eye examinations would be substantially lower for those with diabetes than for those without.2
There is some evidence currently from private and public payers that suggest reducing cost-sharing for targeted high-value services can lead patients to use more of these services, while conversely reducing the use of targeted low-value services.2-4For example, a systematic review in 2018 found improvement in medication adherence with VBID without an increase in total health care spending (implying that increased utilization was offset by decreases in spending for other health care services).4
Source: Center for Value-Based Insurance Design. University of Michigan. http://vbidcenter.org/v-bid-tv.
Used with permission. For more information and resources, check out http://vbidcenter.org
Read more about value-based insurance design:
Precision Benefit Design: Using “Smarter” Deductibles to Better Engage Consumers and Mitigate Cost-Related Non-Adherence
Fendrick MA, Chernew ME. JAMA Internal Medicine. 2017;177(3):368-370.